Professor Harrison Weisinger on Substack → SUBSCRIBE

Your body is sending you a message, and you are not imagining it. The recovery that once took a day now takes three. The weight that shifted with minor dietary adjustments now seems cemented in place. The sharpness you relied on in your thirties — the fast recall, the relentless stamina — has developed an unwelcome lag.

These are not signs of failure. They are signs of biology. Measurable, predictable, and — critically — modifiable.
I have spent more than twenty years in medicine, working with executives, entrepreneurs, and high performers whose livelihoods depend on their bodies and minds functioning at capacity. The conversation I have most often begins the same way: “I just don’t feel like myself lately.” By the time most people arrive in my practice, the changes have been accumulating silently for years. The forties are when the bill arrives.
This article is a clinical map of what is actually happening in the forty-something body — and what the evidence says you can do about it.
Sarcopenia — the progressive loss of skeletal muscle mass and function — does not begin at seventy. It begins in your thirties and accelerates through your forties and fifties. The European Working Group on Sarcopenia revised its definition in 2019 to emphasise that this is not merely an age-related inconvenience but a clinical condition with measurable consequences for metabolic health, physical function, and mortality¹.
The rate of loss is roughly 3–8% per decade after thirty², accelerating after fifty. In practical terms, this means a forty-five-year-old who has not engaged in structured resistance training has already lost a meaningful proportion of the muscle they carried at twenty-five. Grip strength — one of the strongest single predictors of all-cause mortality — declines in parallel. A 2023 meta-analysis of 49 prospective studies (n≈878,000) confirmed the dose-response relationship: muscle wasting is associated with significantly higher all-cause, cardiovascular, cancer, and respiratory mortality, with an inverse linear relationship between muscle mass and death³.

I see this constantly. Patients who were active in their twenties and early thirties drifted away from structured exercise during the years of career building and young families. By their mid-forties, they have lost muscle they do not realise they ever had — and the downstream effects are not subtle: reduced resting metabolic rate, impaired glucose disposal, increased injury risk, and diminished physical resilience.
A 2023 network meta-analysis of 42 RCTs (n=3,728) confirmed that resistance exercise — particularly when combined with nutritional interventions — remains the most effective strategy for reversing sarcopenic decline, with high-certainty evidence for improvements in grip strength, gait speed, and quality of life⁴ (noting that this network meta-analysis included predominantly older adults with confirmed sarcopenia; the direction of effect is expected to apply to midlife prevention, though direct RCT evidence in forty-somethings is limited).
What to do
Resistance training two to four times per week is the cornerstone intervention for preserving muscle mass, metabolic rate, and functional capacity across the lifespan¹. Protein intake must hit the threshold: Morton et al.’s systematic review of 49 RCTs (n=1,863) established the ceiling at approximately 1.62 g/kg/day for fat-free mass gains — hitting it matters, obsessing beyond it does not⁵. The broader therapeutic range of 1.6–2.2 g/kg/day accounts for individual variation, training status, and age-related anabolic resistance. Omega-3 supplementation further supports muscle recovery and reduces exercise-induced inflammation⁶⋅⁷. If you are over forty and not lifting weights, you are losing a war you do not yet know you are fighting. (See the Exercise Prescription box below for the complete training framework.)
Exercise Prescription for the Forty-Something
If you do nothing else in your forties, lift heavy things. Resistance training is not optional — it is the single most important intervention you have. Muscle is the organ of longevity. It regulates glucose, protects joints, stores amino acid reserves for illness, and is the primary driver of your metabolic rate. Two to four sessions per week built around compound movements — squats, deadlifts, rows, presses — with progressive overload is the minimum effective dose. You don’t need to live in a gym. You need to make what you do there count, and you need it to get harder over time.
Your aerobic base matters almost as much. Around eighty percent of your cardiovascular training should be Zone 2 — that comfortable pace where you can hold a full conversation. It feels too easy, and that’s exactly the point. Zone 2 work builds mitochondrial density, improves fat oxidation, and is the foundation of metabolic health. Three to four hours a week of walking, cycling, or easy jogging does more for your long-term health than most people realise. The other twenty percent is where it gets serious. VO₂ max — your body’s ceiling for oxygen utilisation — is among the strongest predictors of all-cause mortality we have, rivalling or exceeding smoking status and blood pressure in some analyses⁸. One to two sessions per week of high-intensity intervals, something like four sets of four minutes at ninety to ninety-five percent of your maximum heart rate, with three minutes of recovery between, will push that ceiling higher. It is uncomfortable. It is also one of the highest-yield investments in longevity you can make.
Here is what almost everyone misses: power. After forty, muscular power — the ability to produce force quickly — declines at roughly twice the rate of strength. This is why you trip, why you can’t react fast enough, why falls become dangerous. Five minutes of plyometric work before your lifting sessions changes the trajectory entirely. Start with countermovement jumps to a soft surface or medicine ball slams — build landing mechanics first. Progress to box jumps after 4–6 weeks. Progress from basic bilateral movements to single-leg and reactive variations over eight to twelve weeks, the way a properly phased system would. The investment is tiny. The return is disproportionate.
And spend five minutes on mobility work daily — it is the boring gap between what your body can do and what it will actually let you do, and ignoring it catches up with everyone eventually.
Muscle Mass: Your Longevity Engine Muscle isn’t just for aesthetics; it’s the organ of longevity, dictating metabolic rate, glucose control, and functional resilience. Sarcopenia starts silently in your thirties, accelerating through midlife with measurable consequences for health and mortality. Resistance training is non-negotiable — it’s the single highest-yield investment you can make to reclaim your biological capital.
Sarcopenia and osteoporosis are not separate problems. They progress together, they share risk factors, and — conveniently — they respond to the same interventions. The resistance training and protein targets already outlined in this article protect bone mineral density as effectively as they protect muscle. A meta-analysis of RCTs in adults aged forty-five and older found that both high-load and low-load resistance training preserve bone mineral density at the femoral neck and lumbar spine⁹. You do not need a separate bone programme. You need the programme you should already be doing.
The scale of the problem is worth stating. NHANES data show that 43.9% of US adults over fifty have low bone mass (osteopenia) or osteoporosis at the femoral neck or lumbar spine ¹⁰. This is not a niche concern for elderly women. It is a population-level reality that begins tracking in midlife.
Screening matters. The USPSTF recommends DXA screening for all women aged sixty-five and older, and for postmenopausal women under sixty-five at increased fracture risk (Grade B)¹¹. For men, the evidence is insufficient for a blanket recommendation, but clinical judgement applies. The practical point: the DEXA scan I recommend for body composition assessment also generates a T-score for bone density. Two readings, one scan. Ask for both.
Testosterone in men declines at approximately 1–2% per year from the age of thirty. This is not a cliff — it is a slope. But slopes compound. By forty-five, a man may have lost 15–30% of the testosterone he carried at his peak¹².
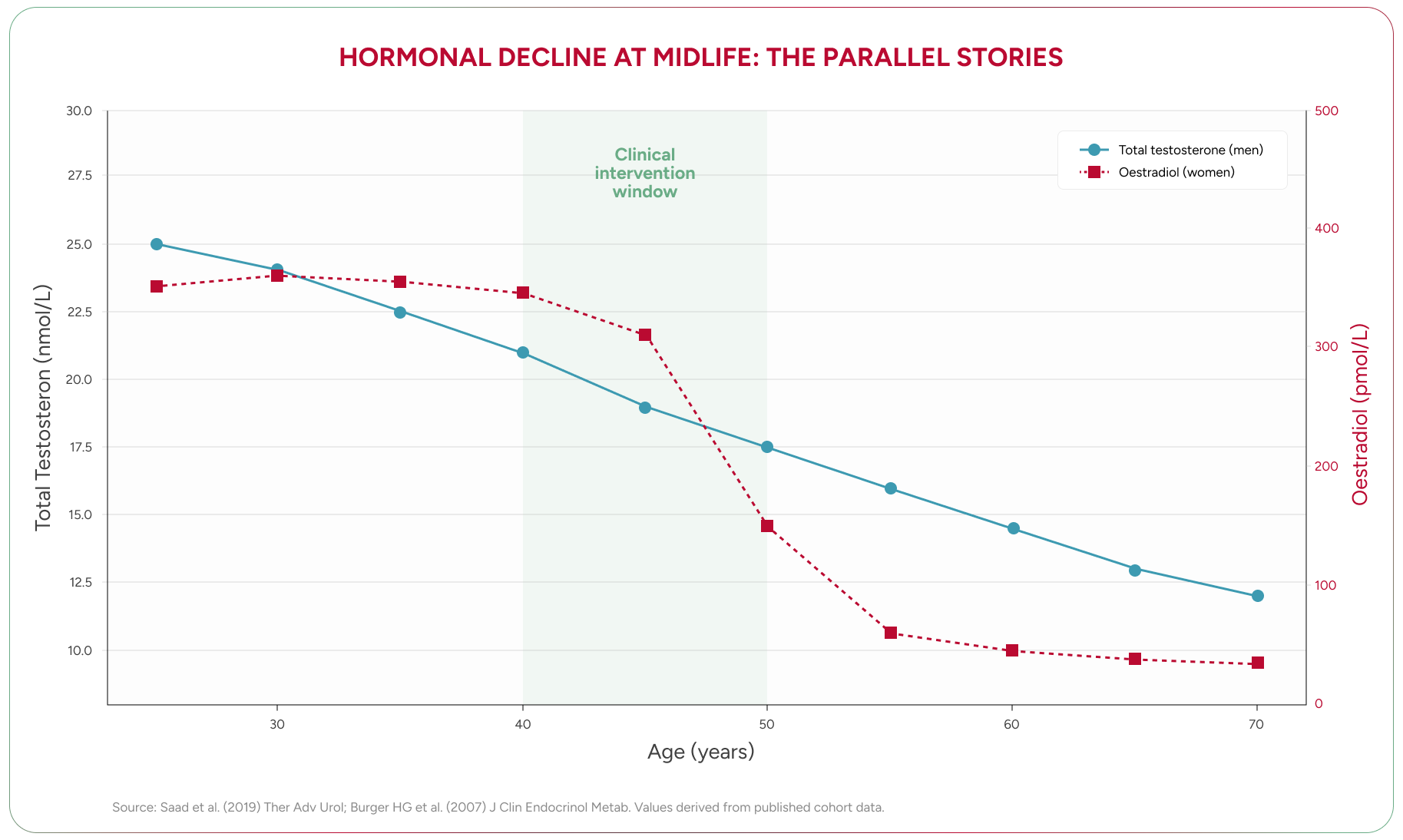
The clinical picture is more nuanced than a single number. Total testosterone — the figure most commonly reported on standard pathology — tells only part of the story. What matters is free testosterone, the fraction that is biologically active and available to tissues. As men age, sex hormone-binding globulin (SHBG) — a protein that binds testosterone and renders it inactive — rises steadily, meaning free testosterone falls faster than total testosterone suggests¹³. A man can have a “normal” total testosterone level and still be functionally deficient.
Men in their mid-forties often describe fatigue and reduced drive without knowing why. Checking the full hormonal panel frequently reveals the answer.
Saad et al. documented that testosterone therapy in men with confirmed deficiency was associated with sustained improvements in body composition, metabolic markers, and quality of life over eleven years of follow-up in a controlled registry study (12). Wu et al. further characterised the hormonal shifts of midlife men, noting that the decline is not limited to testosterone — DHEA, growth hormone, and IGF-1 all follow similar trajectories (13). Livingston and Heald’s 2023 review of adult male hypogonadism reinforced the diagnostic complexity — emphasising the variability of symptoms, the rise of late-onset hypogonadism with age, and the importance of standardised testosterone testing protocols to avoid misclassification¹⁴.
An important caveat on cognition: while testosterone replacement reliably improves body composition and metabolic markers, a 2019 systematic review and meta-analysis of 21 randomised controlled trials found no significant improvement in overall cognitive functioning (Hedges’ g = 0.09, p = 0.108) — no measurable benefit for processing speed, verbal or visual memory, working memory, executive function, or overall cognitive status¹⁵. This matters because cognitive decline is a common concern driving men toward TRT. The body composition benefits are real. The cognitive benefits, as yet, are not supported by the evidence. Honest science requires saying so.
What to do
Testosterone: Beyond the Numbers The gradual decline of testosterone in men is nuanced; free testosterone, not just total, dictates biological availability. A ‘normal’ total level can mask a functional deficiency due to rising SHBG. While lifestyle optimization is paramount, targeted testosterone therapy offers genuine body composition benefits, though its cognitive impact remains unproven by evidence.
Testosterone gets the headlines. But the most consequential hormonal shift of midlife is the one that remains systematically under-recognised — and it affects half the population.
Perimenopause — the transitional phase before menopause — typically begins in the early to mid-forties, though it can start as early as the late thirties. It is, in my clinical experience, the most under-treated hormonal transition in medicine.
The reason is simple: the symptoms are varied and non-specific. Insomnia. Anxiety. Brain fog. Joint pain. Irritability. Weight gain. Reduced stress tolerance. Loss of confidence. These are frequently attributed to burnout, depression, or “just getting older.” I regularly see women who have been prescribed antidepressants, anxiolytics, and sleep medications when the underlying driver was fluctuating and declining oestradiol.
Oestrogen is not merely a reproductive hormone. It is neuroprotective, cardioprotective, and metabolically active. Its decline affects virtually every organ system. The American Heart Association’s 2020 scientific statement on the menopause transition confirmed that perimenopause is a critical inflection point for adverse metabolic and vascular changes — increased dyslipidaemia, insulin resistance, and cardiovascular disease risk — reinforcing the case for early screening and intervention rather than waiting for menopause to declare itself¹⁶. The evidence base for hormone replacement therapy (HRT) has shifted substantially in recent years. The 2002 Women’s Health Initiative findings — which led to a generation of women and their doctors avoiding HRT — have been extensively re-analysed. The current consensus, supported by the British Menopause Society, the Australasian Menopause Society, and the North American Menopause Society, is that for symptomatic women initiating HRT within ten years of menopause onset, the benefits substantially outweigh the risks. This generalisation does not apply to women with a history of hormone-sensitive cancer, unexplained vaginal bleeding, active liver disease, or prior thromboembolic events, who require individualised assessment.
Manson et al.’s 18-year follow-up of the WHI trials (n=27,347 women) put numbers to this: HRT was not associated with increased all-cause mortality (HR 0.99, 95% CI 0.94–1.03), cardiovascular mortality (HR 1.00), or cancer mortality (HR 1.03). Among younger women aged 50–59, those on HRT had approximately 30% lower death rates during the intervention phase¹⁷ — in absolute terms, roughly 6 fewer deaths per 1,000 women over the 7-year intervention period, a clinically meaningful reduction that reframes the risk-benefit conversation entirely (the WHI enrolled postmenopausal women aged 50–79; the timing hypothesis — that earlier initiation confers greater benefit — is supported by subgroup analyses but has not been tested in a dedicated RCT of perimenopausal women). The fear that persists in many consulting rooms is not supported by the long-term data.
What to do
Oestrogen: The Unseen Architect Perimenopause, often misdiagnosed and undertreated, is a profound hormonal shift beginning in the early forties, impacting brain, heart, and metabolism. Modern evidence supports body-identical HRT for symptomatic women, with benefits decisively outweighing risks. The critical window for intervention is perimenopause itself — not menopause.
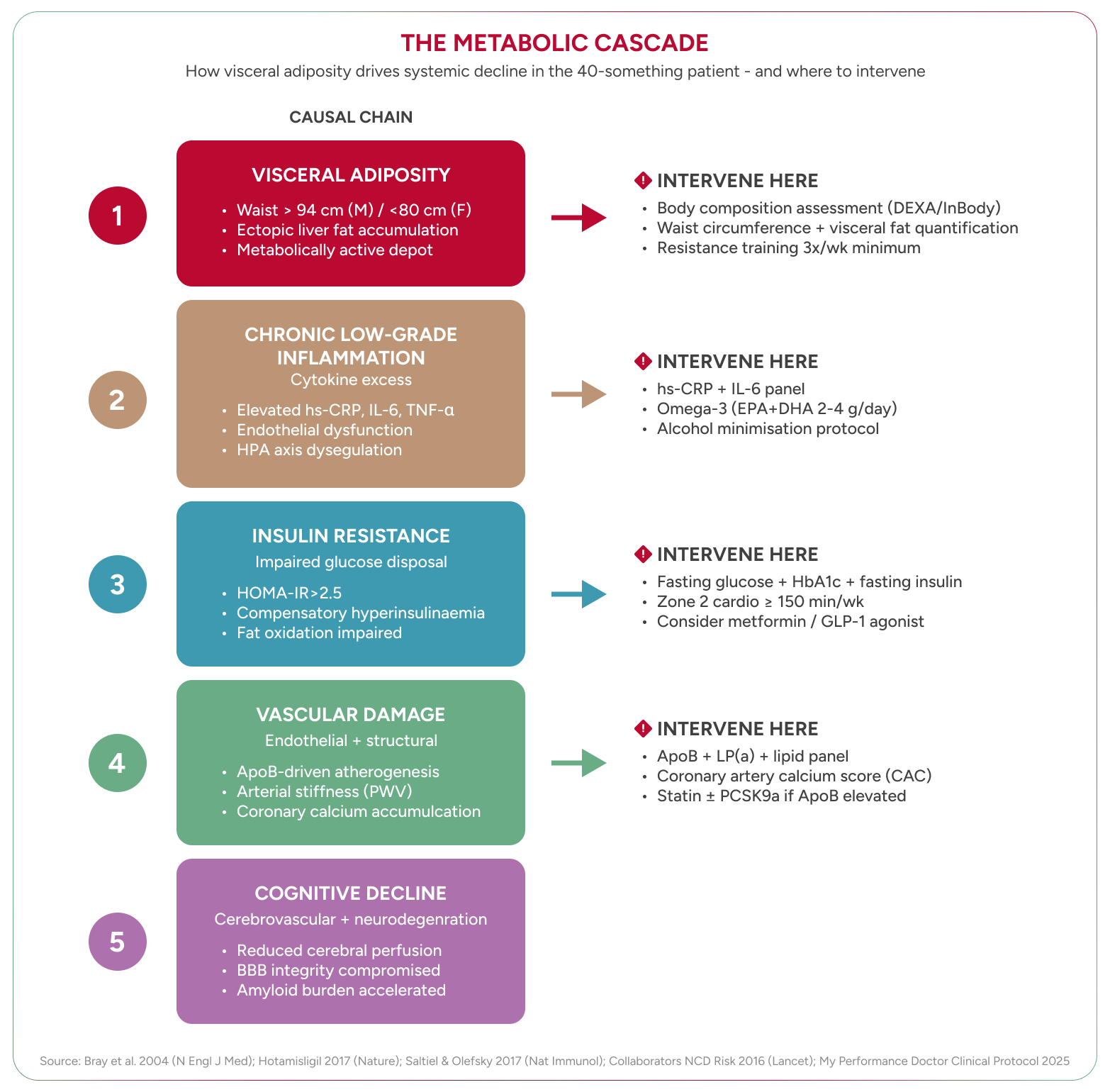
Hormonal decline does not happen in isolation — it reshapes how your body stores and burns energy. The metabolic rate does decline with age, but not for the reason most people assume. The primary driver is not some mysterious slowing of cellular machinery. It is the loss of metabolically active tissue: muscle. Every kilogram of muscle lost reduces resting energy expenditure. The body does not slow down arbitrarily. It slows down because its engine has shrunk.
Simultaneously, body composition shifts. Subcutaneous fat — the fat beneath the skin — gives way to visceral fat, the metabolically active fat that surrounds the abdominal organs. Visceral fat is not inert storage. It is an endocrine organ that secretes inflammatory cytokines, disrupts insulin signalling, and drives the chronic low-grade inflammation — sometimes termed “metaflammation” — that Hotamisligil identified as a central mechanism linking obesity to metabolic disease¹⁹.
Aguilar et al. found that metabolic syndrome — the clustering of central obesity, dyslipidaemia, hypertension, and impaired glucose regulation — affects more than a third of American adults, with prevalence rising sharply in the forties²⁰. HOMA-IR — a measure of how resistant your cells have become to insulin — rises well before fasting glucose becomes abnormal²¹. By the time a standard blood test flags “pre-diabetes,” insulin resistance has been present for years.
What to do
Nutritional priorities for the forty-something
Metabolic Reset: Your Command Centre Midlife isn’t about mysterious decline; it’s a call to reclaim your metabolic command. Combat muscle loss and visceral fat directly, leveraging precise diagnostics like OGTT for early intervention. This is not about dieting, but about strategically recalibrating your body’s engine for sustained performance and longevity.
The Visceral Shift: Reclaiming Metabolic Control Your metabolic rate slows because your muscle engine shrinks, not mysteriously. Visceral fat isn’t passive; it’s an inflammatory factory driving insulin resistance years before diagnosis. Aggressive monitoring and a ruthless focus on metabolic quality—not mere calorie counting—are your weapons.
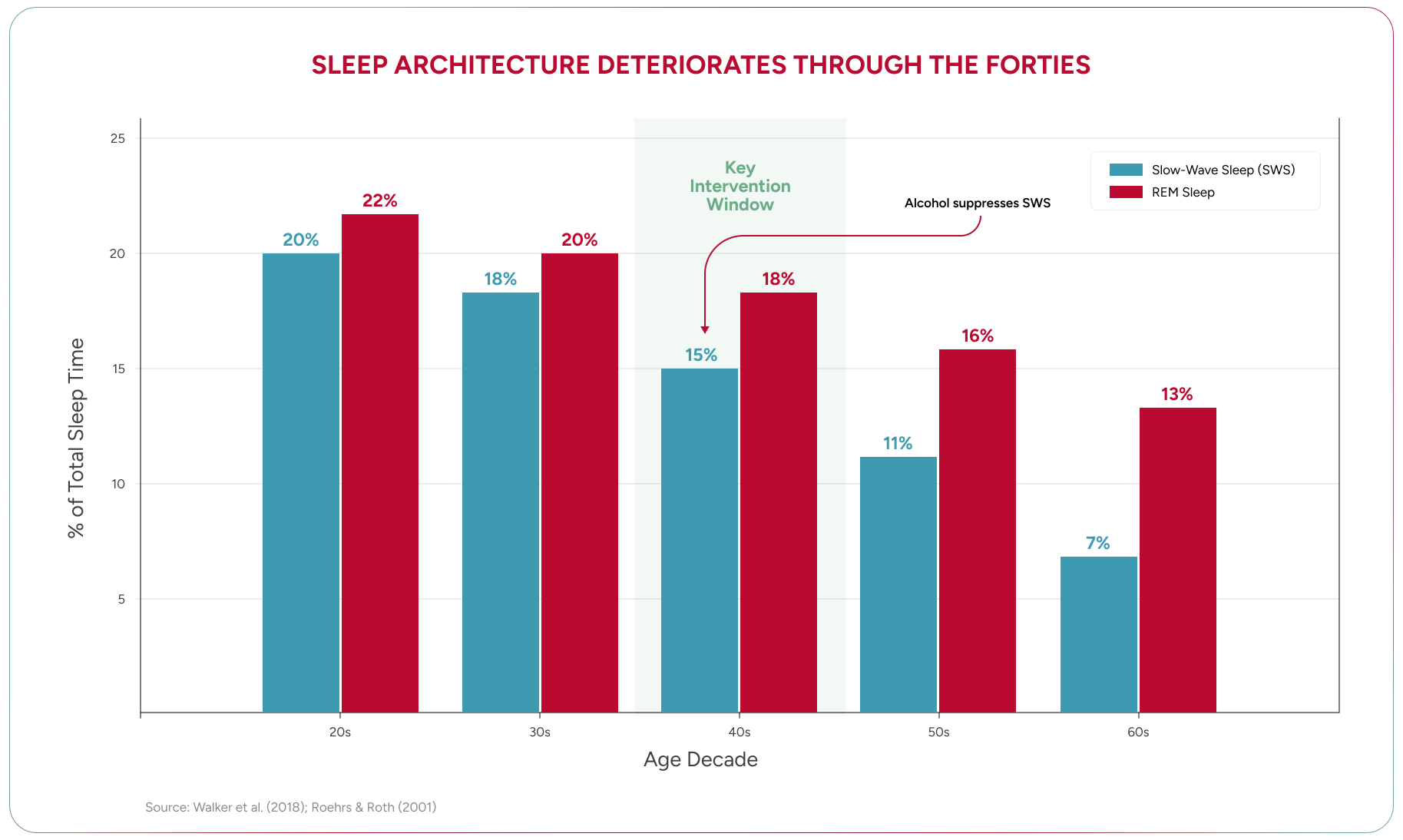
Sleep does not simply get “lighter” with age. Its architecture changes in specific, measurable ways. Slow-wave sleep — the deep, restorative phase during which growth hormone is secreted, memories are consolidated, and cellular repair occurs — declines significantly from the mid-thirties onward²².
Wilckens et al. reviewed the evidence that slow-wave activity is directly linked to cognitive performance — its loss impairs memory consolidation, executive function, and the restorative processes the forty-something brain depends on²². Growth hormone secretion, which occurs predominantly during slow-wave sleep, falls in tandem. The relationship is bidirectional: poor sleep reduces growth hormone, and reduced growth hormone impairs sleep quality.
Alcohol is the most common sleep disruptor I see, and the most consistently underestimated. Patients tell me alcohol “helps them sleep.” It does not. Alcohol is a sedative — it induces unconsciousness, which is not sleep. It suppresses REM sleep, fragments sleep architecture, and eliminates much of the restorative slow-wave activity that the forty-something brain desperately needs. Roehrs and Roth’s canonical review documented the biphasic effect: alcohol may induce sedation in the first half of the night, but the second half is characterised by REM suppression, fragmentation, and autonomic arousal — the net effect is worse sleep, not better²³. You cannot adapt to sleep restriction. The evidence on this point is consistent and strong.
What to do
Prioritise seven to eight hours of sleep opportunity, not just time in bed. Establish a consistent sleep-wake schedule — including weekends. Eliminate or dramatically reduce alcohol, particularly within three hours of sleep. Screen for obstructive sleep apnoea (OSA), which is significantly under-diagnosed in the forty-to-sixty demographic, particularly in women. The HypnoLaus study (n=2,121) found that 49.7% of men and 23.4% of women had moderate-to-severe sleep-disordered breathing — prevalence figures substantially higher than previously recognised, largely because earlier studies used less sensitive recording methods²⁴. Wearable sleep trackers — while imperfect — provide useful longitudinal data. The Epworth Sleepiness Scale remains a validated screening tool for excessive daytime somnolence — a score of 10 or above warrants further evaluation²⁵).
The forties are the pivotal decade for cardiovascular risk — not because heart attacks are common at forty-five, but because the atherosclerotic plaque that causes the heart attack at fifty-five is being laid down now. This is the window where intervention has the greatest leverage.
The traditional lipid panel — total cholesterol, LDL, HDL, triglycerides — is necessary but insufficient. ApoB — apolipoprotein B, a direct measure of the number of atherogenic lipoprotein particles circulating in your blood — is a superior predictor of cardiovascular events. You can have a “normal” LDL-cholesterol and an elevated ApoB. The particles, not the cholesterol content, drive plaque formation. Sniderman et al.’s review in JAMA Cardiology laid this out clearly: each atherogenic lipoprotein particle contains exactly one ApoB molecule, making ApoB a direct count of total atherogenic particle number — it “unifies, amplifies, and simplifies” cardiovascular risk assessment versus LDL-C or non-HDL-C alone²⁶. The 2024 National Lipid Association Expert Clinical Consensus (Soffer et al.) went further, formally recommending ApoB measurement for cardiovascular risk management in adults — elevating it from a useful adjunct to a guideline-endorsed standard for improved risk stratification, particularly in middle age²⁷.
Lipoprotein(a) — Lp(a) — is a genetically determined, largely unmodifiable cardiovascular risk factor that approximately 20% of the population carries at elevated levels²⁸. It should be measured once in every adult’s lifetime. If it is elevated, the management of all other modifiable risk factors becomes more aggressive.
Coronary artery calcium (CAC) scoring — a low-dose CT scan that quantifies the calcium deposited in coronary artery walls — provides a direct visualisation of subclinical atherosclerosis. A CAC score of zero at forty-five is powerfully reassuring. A non-zero score at forty-five demands action.
High-sensitivity C-reactive protein (hs-CRP) reflects systemic inflammation and provides additional risk stratification beyond lipid markers. Hotamisligil’s work demonstrated the mechanistic link between chronic inflammation, metabolic dysfunction, and vascular disease¹⁹.
A CAC score of zero at forty-five is reassuring. It is not definitive. Studies using coronary CT angiography and carotid ultrasound consistently demonstrate that 70–86% of patients with a zero CAC score harbour non-calcified — “soft” — plaque that calcium scoring cannot see²⁹. This matters because soft plaque is the substrate of acute coronary events. Calcified plaque is stable. It is the non-calcified, lipid-rich plaque that ruptures.
Carotid plaque detection by ultrasound — not carotid intima-media thickness (CIMT) measurement, which has been appropriately downgraded as a standalone predictor — adds independent prognostic value. The Mannheim Consensus (2012) drew this distinction clearly: plaque presence and CIMT are separate phenotypes, and plaque presence is the one that matters²⁹. The ARIC study (Nambi et al., n=13,145) demonstrated that adding carotid plaque assessment to traditional risk factors reclassified 23% of subjects into different risk categories, with a net reclassification improvement of 9.9%³⁰. For the forty-something with a zero CAC score and residual risk factors, carotid ultrasound provides a radiation-free, low-cost window into soft plaque burden that calcium scoring misses. It does not replace the CAC score. It complements it — particularly in younger cohorts where calcification has not yet declared itself.
The more striking advance is the Perivascular Fat Attenuation Index. The Fat Attenuation Index (FAI) is a CT-derived biomarker that detects coronary artery inflammation by measuring changes in the adipose tissue immediately surrounding the coronary arteries — perivascular fat. When a coronary artery is inflamed, the inflammation inhibits normal lipid accumulation in adjacent fat, shifting its CT attenuation in a measurable, quantifiable way. This is not anatomy. This is biology — active vascular inflammation, detected non-invasively from a standard CT scan.
The CRISP-CT study (Oikonomou et al., Lancet, 2018, n=3,912) was the landmark: an elevated perivascular FAI around the right coronary artery predicted cardiac mortality with a hazard ratio of 9.0 — independent of calcium score, traditional risk factors, and high-risk plaque features³¹. To calibrate that number: baseline cardiac mortality in these cohorts is low (roughly 1–2 per 1,000 patient-years), so a ninefold increase represents a shift from very low to low-but-clinically-significant absolute risk — the kind of signal that justifies aggressive primary prevention, not panic. The ORFAN study (Chan et al., Lancet, 2024, n=40,091) confirmed and extended this finding: among patients with no or minimal obstructive coronary artery disease, those with the highest FAI scores had 9.5 times the cardiac mortality risk, with events predicted up to ten years in advance³². Again, these are relative risks applied to a low-baseline-rate population — the absolute numbers remain small, but the discriminative power is what matters for identifying who needs earlier, more aggressive intervention. A meta-analysis of 7,797 patients across 20 studies reported a pooled hazard ratio of 3.29 for major adverse cardiac events in those with elevated FAI³¹.
This matters because it identifies a fundamentally different axis of risk. Your calcium score tells you how much plaque has calcified. The FAI tells you whether your coronary arteries are actively inflamed right now — and it is that inflammation that makes otherwise stable-looking plaque rupture. Patients with structurally normal-appearing vessels on standard imaging can carry profound inflammatory risk that only this analysis detects.
_%20DETECTING%20CORONARY%20INFLAMMATION.png)
Two additional points are clinically important. First, FAI-detected coronary inflammation is modifiable — statin therapy has been shown to reduce perivascular fat attenuation, providing a direct, measurable therapeutic target³¹. Second, the clinical implementation of FAI analysis — the CaRi-Heart scan, developed from the Oxford research programme — is now available privately in Australia. It is not yet guideline-endorsed by the ACC/AHA, ESC, or CSANZ, and it is not Medicare-rebatable. But the evidence base is compelling and growing, and for the motivated individual seeking the most complete picture of their coronary risk, it represents a genuinely novel tool.
What to do
Request ApoB, Lp(a), and hs-CRP in addition to a standard lipid panel. Discuss a CAC score with your medical practitioner if you have any risk factors — family history, hypertension, smoking history, diabetes, or elevated Lp(a). If your CAC score returns at zero but you carry residual risk factors, consider carotid plaque ultrasound — a radiation-free assessment that detects the soft plaque calcium scoring misses. For those seeking the most complete coronary risk picture, the CaRi-Heart scan (FAI analysis from a standard coronary CT angiogram) can identify active coronary inflammation independent of plaque burden — ask your cardiologist whether it is appropriate for your risk profile. Monitor blood pressure at home, not just in clinic. Statin therapy, when clinically indicated, has one of the strongest evidence bases of any cardiovascular intervention. The decision should be made on clinical grounds, not on the basis of online commentary.

Every system discussed so far — metabolism, hormones, sleep, cardiovascular health — converges on a single organ. The brain is not exempt from these changes. It is their primary casualty.
Foret et al. found that executive function scores — the cognitive domain responsible for planning, decision-making, and impulse control — declined with each additional metabolic syndrome component (β=−0.14, p=.044) in adults aged forty to sixty³³. In practical terms, the more cardiovascular risk factors you carry, the slower and less sharp your thinking becomes.
Ye et al. (2024), drawing on the PATH Through Life study, confirmed that physical activity in midlife was associated with preserved cognitive function over a twelve-year follow-up³⁴.
The mechanisms are well characterised. Hötting and Röder reviewed the evidence for exercise-induced neuroplasticity — increased BDNF (brain-derived neurotrophic factor), hippocampal neurogenesis, improved cerebrovascular function, and reduced neuroinflammation³⁵. Colcombe and Kramer’s meta-analysis of randomised controlled trials demonstrated that aerobic exercise produced reliable improvements in executive function, with the largest effects in those over fifty — suggesting that the intervention becomes more, not less, important with age³⁶.
The longitudinal data is equally compelling. Yaffe et al. followed 5,925 women over six to eight years and found that those who were more physically active at baseline experienced significantly less cognitive decline³⁷. Whitmer et al. demonstrated that midlife physical activity was associated with a substantially reduced risk of dementia decades later³⁸. The broader evidence consistently supports the association between midlife physical activity and reduced dementia risk. The 2020 Lancet Commission on dementia prevention identified physical inactivity as one of twelve modifiable risk factors, estimating that addressing all modifiable factors could prevent or delay up to 40% of dementia cases worldwide³⁹. The protective effect is strongest when exercise is established in the forties and fifties — exactly the window most people let it lapse. Gallaway et al. synthesised the broader evidence base, concluding that regular exercise is the single most effective non-pharmacological intervention for preserving cognitive function across the lifespan⁴⁰.
Sleep, too, exerts an independent and powerful effect on long-term cognitive risk. Xu et al.’s systematic review of 51 longitudinal cohorts quantified the relationship: short sleep and sleep disturbance were associated with increased risk of cognitive decline and all-cause dementia, while insomnia and sleep-disordered breathing further compounded the risk⁴¹. The sweet spot — seven to eight hours — is not a lifestyle preference. It is a dose-response relationship with neurodegeneration.
Sonnenburg and Bäckhed identified the gut microbiome as a mediator between metabolic health and systemic inflammation, with implications for neuroinflammation and cognitive function⁴². The gut-brain axis is not peripheral to the clinical picture — it is central to it, and an active area of research with direct relevance to the metabolically stressed forty-something.
What to do
Protect your brain by protecting your metabolism. Aerobic exercise, resistance training, sleep, and metabolic health optimisation are not separate interventions — they are the same intervention, viewed from different angles. If you are noticing cognitive changes in your forties, do not attribute them to age alone. Investigate the metabolic, hormonal, and sleep-related contributors first.
So if the science is clear and the interventions are available, why do so many smart, driven people arrive at forty already behind? The answer lies in the decade that preceded it.
The thirties are, for most high performers, the decade of maximum compression. Career acceleration. Business building. Relationship formation. Children. Financial pressure. Every domain demands more, simultaneously. Something gives — and it is almost always the body.
Exercise becomes sporadic. Sleep is sacrificed for productivity. Nutrition defaults to convenience. Alcohol increases as a stress management tool. Preventive health screening is deferred because “I feel fine.”
By the time you reach forty, you have spent a decade running down biological capital without reinvesting. The forties are when the account sends its first statement.
I do not say this to assign blame. The squeeze is structural, not moral. The demands are real. But the physiological consequences are equally real, and they compound. The executive who stopped training at thirty-two and resumed at forty-four has lost twelve years of muscle maintenance, metabolic conditioning, and cardiovascular protection. That gap is recoverable — but it requires deliberate, sustained effort.
The Thirty-Something Squeeze: Your Biological Balance Sheet The thirties represent a decade of biological debt for many high performers. Sacrificed sleep, sporadic exercise, and neglected nutrition silently erode metabolic and physical capital. The forties are not a sudden collapse, but the inevitable reckoning – demanding deliberate, sustained action to reclaim what was lost.
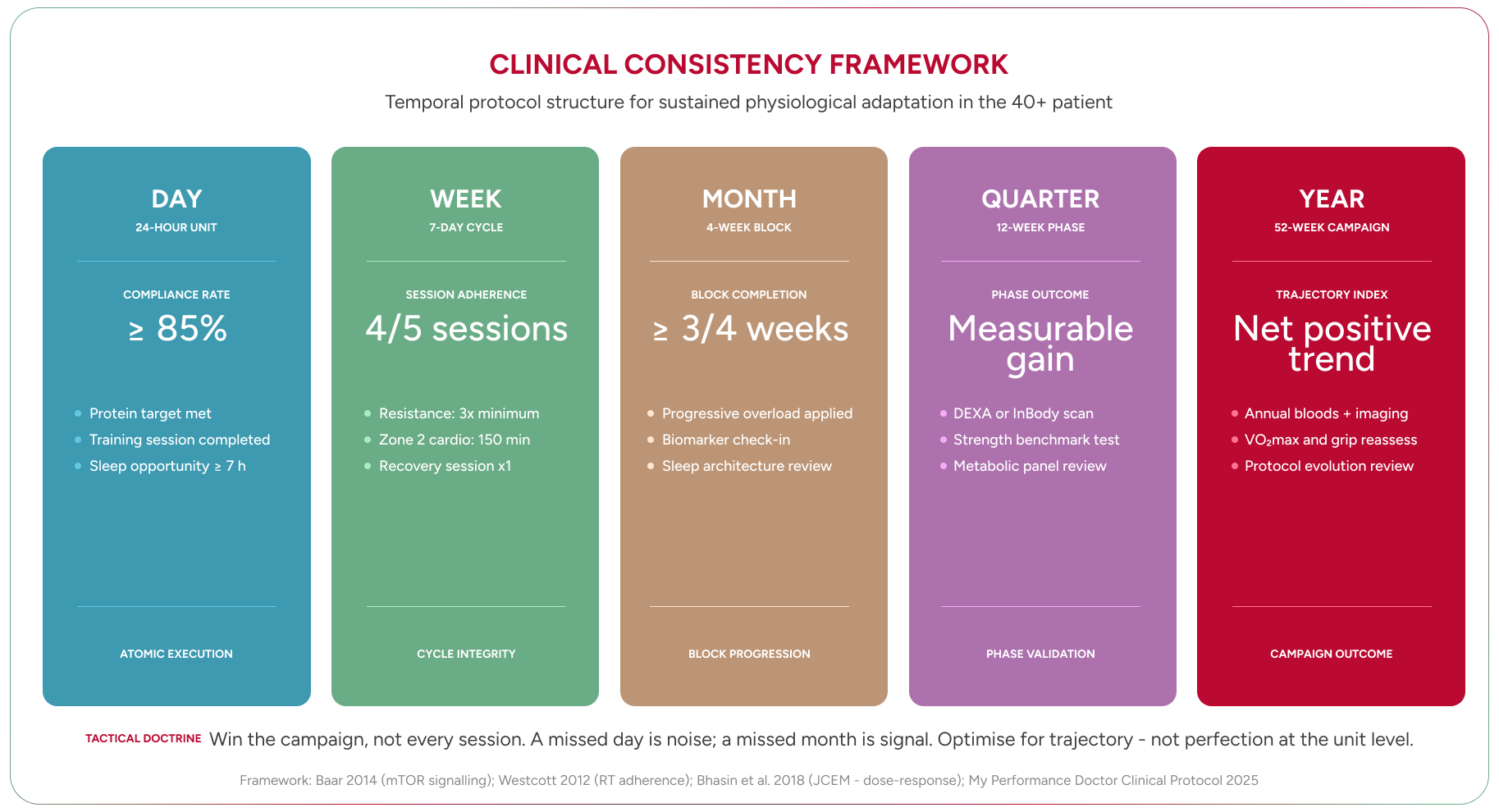
The patients who actually reverse the trajectory of their forties share a common trait. It is not discipline in the conventional sense. It is a framework for consistency.
Perfection is the enemy of progress in health, just as it is in business. The executive who trains four times a week for forty-eight weeks will always outperform the one who trains six times a week for twelve weeks before burning out. The question is never “Did I win today?” It is “Did I win the week?”
Win the week. Then win the month. Then win the quarter. This is how sustainable change is built — in blocks, not in bursts.
A bad day is irrelevant. A bad week is a data point. A bad month is a pattern that requires intervention. This framework — borrowed, deliberately, from the way my patients think about business performance — removes the emotional volatility from health management and replaces it with systems thinking.
The forty-something body is not in decline. It is in transition. And the difference between those who age well and those who do not is rarely genetic. It is architectural — the structures, systems, and habits that either protect biological capital or allow it to erode.
You cannot stop ageing. But you can decide what kind of fifty-year-old, sixty-year-old, seventy-year-old you become — and that decision is being made right now, whether you are making it deliberately or not. The evidence base is robust. The interventions are available. The only question left is whether you will treat your body with the same strategic rigour you bring to everything else that matters. Because the body keeps score. And the forties are when it starts reading the tally out loud.
Final Word: The Gold Standard Longevity isn’t a genetic lottery; it’s an architectural choice. Consistency, not perfection, dictates the biological capital you carry into later decades. The score is being kept, and your strategic decisions now define your future.
I would be doing my patients a disservice if I wrote an article about body composition in the forties without acknowledging that the pharmacotherapy landscape has changed. GLP-1 and dual GLP-1/GIP receptor agonists — semaglutide and tirzepatide — are now approved treatments for obesity, not just diabetes. The trial data are substantial: the STEP 1 trial demonstrated 14.9% mean body weight reduction with semaglutide 2.4 mg over 68 weeks in non-diabetic adults (n=1,961)⁴³, and SURMOUNT-1 showed 20.9% with tirzepatide 15 mg over 72 weeks (n=2,539)⁴⁴. These are not marginal effects. They are transformative.
The Endocrine Society guideline recommends pharmacotherapy as an adjunct for adults with a BMI of 30 or above, or 27 or above with weight-related comorbidities, when lifestyle intervention alone is insufficient⁴⁵. That guideline dates from 2015 and predates both of these agents — an updated clinical practice guideline is expected.
Here is what matters for the readers of this article: weight lost on GLP-1 therapies is not all fat. Neeland et al.’s 2024 review found that 15–60% of weight lost across GLP-1 trials was lean mass⁴⁶. For someone in their forties already losing muscle, that is a clinically important consideration. The mitigation is the same intervention this entire article prescribes — resistance training. If you are on or considering these medications, structured resistance exercise is not optional. It is the difference between losing weight well and losing the muscle you cannot afford to lose.
These are clinician-initiated conversations, not self-prescriptions. Discuss them with your doctor.
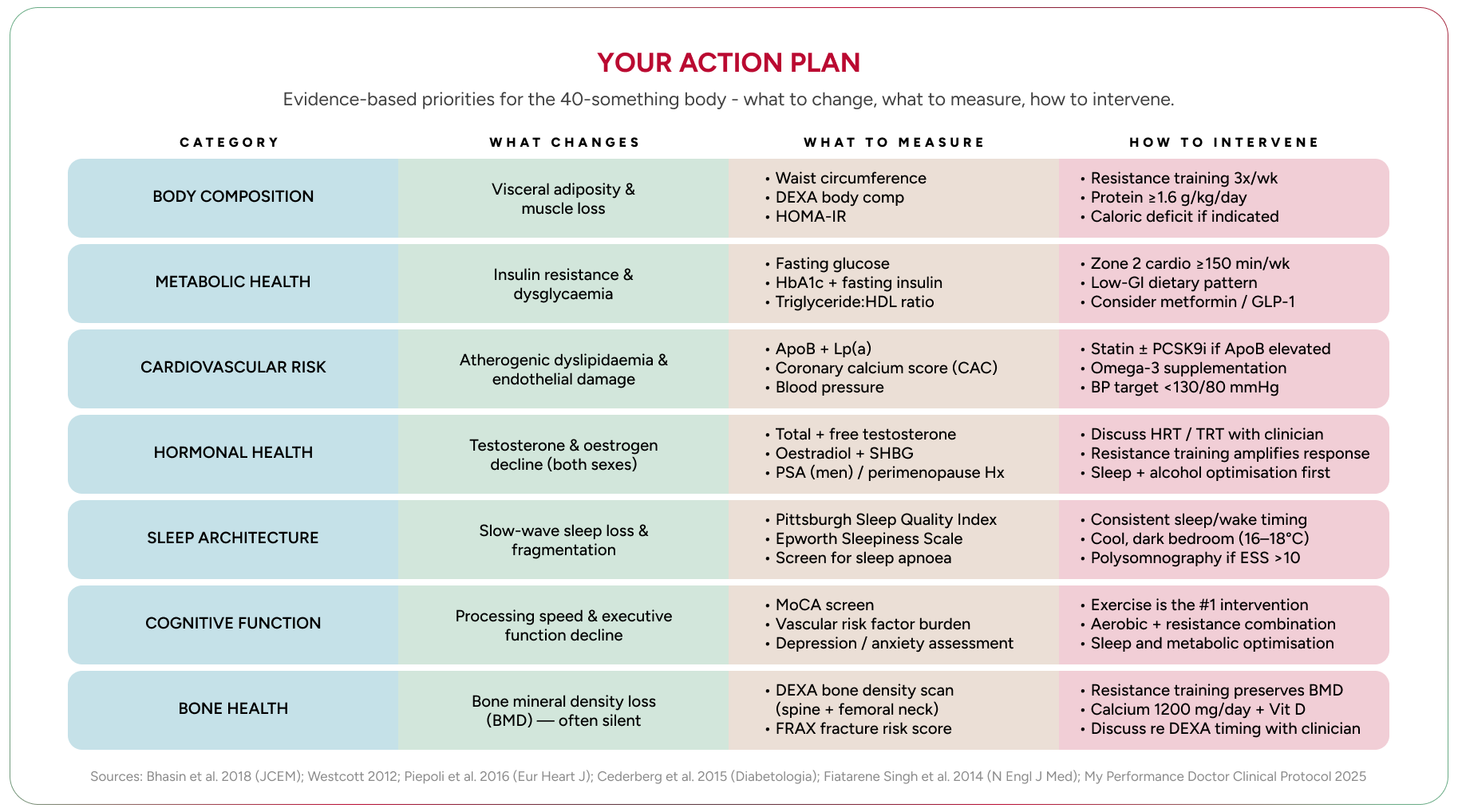
Action Plan: Your Forty-Something Reset The forties are not a decline; they are a demand for strategic intervention. Reclaim your metabolic, hormonal, and physical capital with precision. Act now: your biology is keeping score.
Bone Health | Bone mineral density declines in parallel with muscle mass from midlife | DEXA scan (T-score alongside body composition) | Resistance training (your existing programme covers this); calcium and vitamin D; discuss screening timing with your clinician |


For all media enquiries, please contact press@myperformancedoctor.com
