Professor Harrison Weisinger on Substack → SUBSCRIBE

A guide to perimenopause, hormones, heart health, and taking back control.

There is a sentence I hear more than any other in my practice. It comes from women in their late thirties, forties, and fifties who run companies, manage households, and hold entire ecosystems together. The sentence is always some variation of: “I just don’t feel like myself.”
Then a constellation of symptoms. Waking up tired. Brain fog. Weight gain despite the same diet. Aching joints. Sleep that fractures at 3am. Anxiety out of nowhere. Sex that’s become painful, or without sensation, or accompanied by a libido that’s left the building.
What’s happening is the most complex physiological transition of the human lifespan, landing during what is often the highest-load period of their lives. The medical system has been catastrophically bad at recognising it, naming it, and treating it [1, 2].
The problem isn’t individual doctors. It’s that the system was built around inadequate evidence, and a lot of patients have been caught in the gap between what we knew then and what we know now. A woman feeling terrible at 45 may have been told it’s normal ageing, because until recently that was the consensus.
She may have been prescribed an antidepressant for new-onset anxiety, because without hormonal context that’s a reasonable clinical response. She may have avoided HRT, because the fear generated by a badly reported 2002 study ran deep and took two decades to unpick. And if she raised sexual health, she may have found the conversation moved on, not from indifference, but rather because most clinicians weren’t trained to address it. The evidence has shifted significantly. This article is the clinical map I should have been giving my patients 10 years ago.
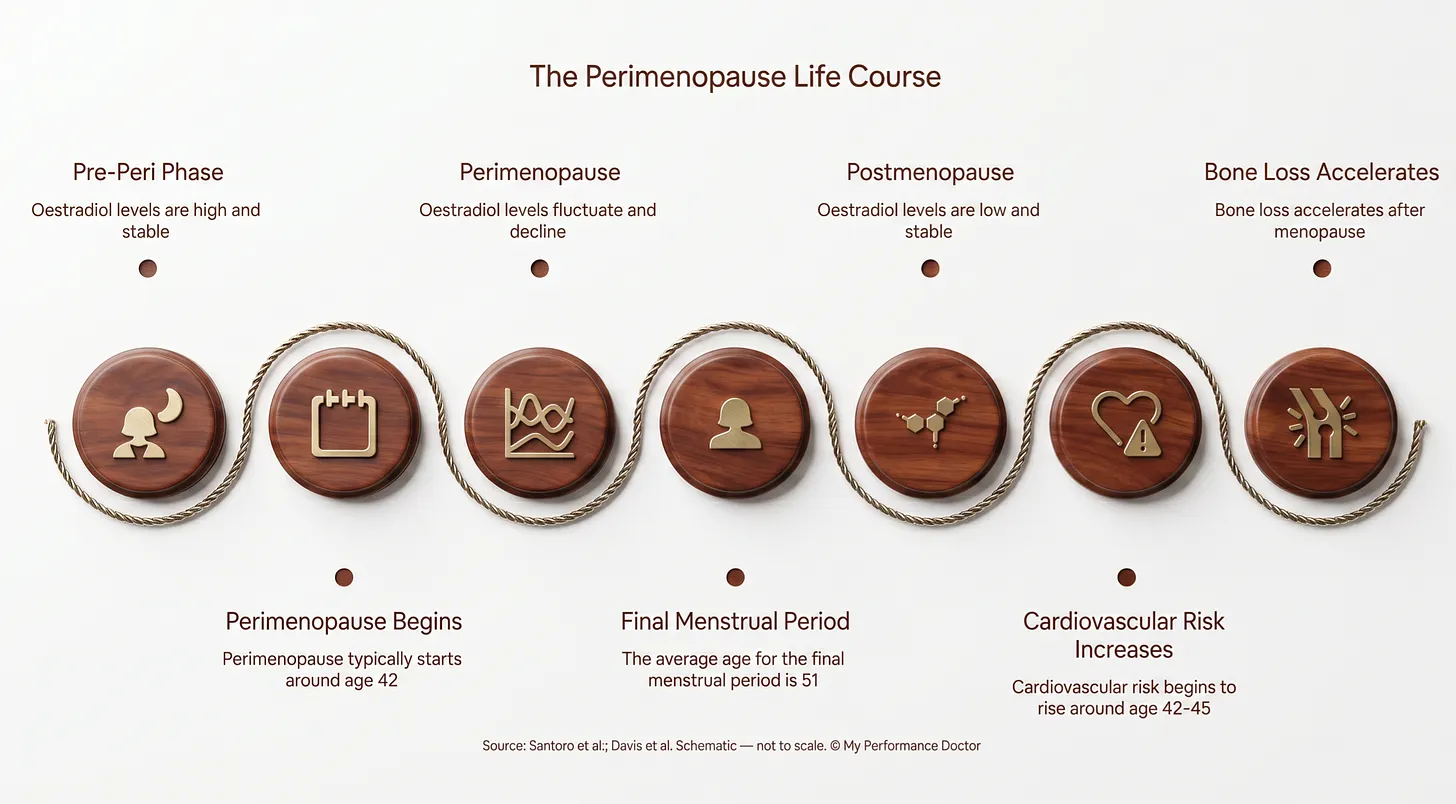
Perimenopause is not menopause’s gentle prelude. It is hormonal chaos.
The textbooks describe menopause as the cessation of ovarian function. What they underplay is the transition: five to ten years before that final period when oestrogen levels fluctuate wildly. One week your oestradiol might be higher than in your twenties. The next, it crashes. This typically begins in the early-to-mid forties but can start in the late thirties [1, 3, 4]. Brinton’s work describes perimenopause as a neurological transition state, driven by oestrogen fluctuation and disrupted glucose metabolism in the central nervous system [1].
Oestrogen is not just a reproductive hormone. It has receptors in virtually every organ system: brain, heart, bone, gut, skin, immune system, vasculature, vaginal and urethral epithelium [4, 5]. When oestrogen fluctuates unpredictably, the effects are systemic. This is why perimenopause presents as everything, everywhere, all at once.
The metabolic consequences arrive early. The ZOE PREDICT study (n=1,002) showed postmenopausal women had 42% higher postprandial glucose responses, 6% higher fasting glucose, and 5% higher HbA1c compared to premenopausal women [2]. Metabolic syndrome prevalence increases sharply: postmenopausal women are two to three times more likely to develop it [1, 7]. The adipose tissue phenotype itself changes, with visceral fat accumulating preferentially, independent of total weight gain [3].
Why is perimenopause so often missed? The symptoms are non-specific, women are socialised to push through, and much of medicine still treats perimenopause as hot flushes and nothing more. Hot flushes are the tip of the iceberg. By the time they arrive (if they arrive at all, as roughly 20% of women never get them), years of hormonal instability have already been reshaping cardiovascular, metabolic, cognitive, and immune function [4, 8].
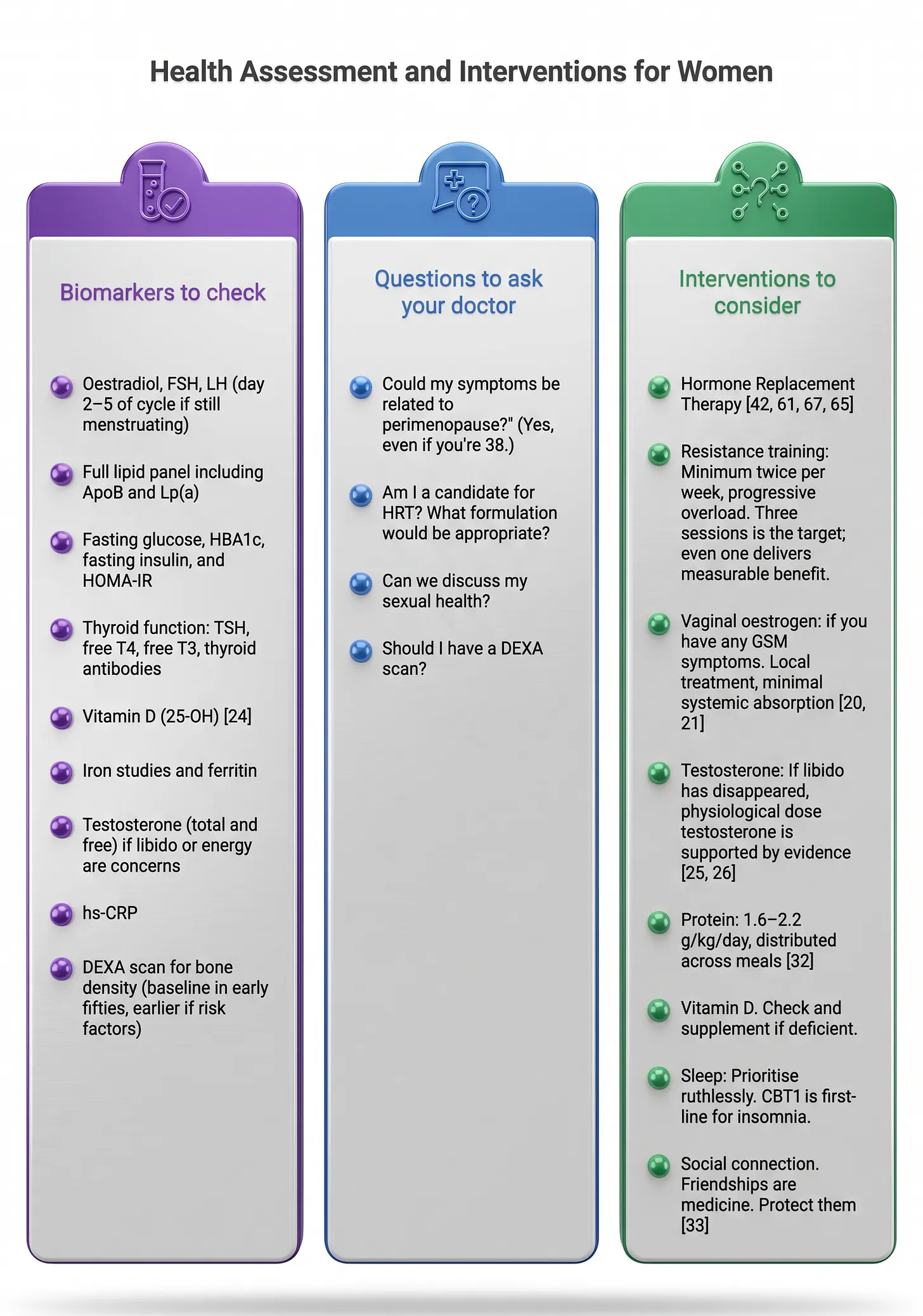
What to consider: If these symptoms are familiar, a clinical assessment is worth raising with your doctor. A useful panel includes oestradiol, progesterone, FSH, testosterone (total and free), and SHBG. If still menstruating, day 2-5 of the cycle gives the most useful baseline. The clinical picture matters more than any single number during perimenopause. Tracking symptoms across two or three cycles before an appointment can be genuinely helpful.
Cardiovascular disease is the leading cause of death in women. Menopause is the inflection point [1, 9].
Liu and colleagues analysed 921,517 participants across 20 cohort studies: women with premature menopause (before age 40) had a relative risk of 1.52 for coronary heart disease, 1.27 for stroke, and 1.36 for total cardiovascular events. Even early menopause (age 40-45) conferred elevated risk [4]. LDL rises 10-15% postmenopause; HDL drops; hypertension becomes twice as common [1, 10].
Heart disease presents differently in women, and this is where the system fails them most dangerously. Women are more likely to experience breathlessness, nausea, back pain, and fatigue than classic crushing chest pain during a myocardial infarction [5]. They are more likely to be misdiagnosed. Less likely to receive angiography, cardiac enzymes, or cardiology referral [9, 11]. Women develop conditions rarely seen in men (MINOCA, SCAD, takotsubo cardiomyopathy) that require entirely different diagnostic frameworks [6].
Thurston’s SWAN data added something clinicians should sit with: vasomotor symptoms are associated with subclinical cardiovascular disease, including greater carotid intima-media thickness and coronary artery calcification [7]. The hot flush is a signal.
What to consider: A cardiovascular baseline including ApoB, Lp(a), hs-CRP, and a lipid panel can be useful to establish where you’re starting from. Blood pressure is worth tracking at home if you haven’t already. If there’s a family history of heart disease, premature menopause, or PCOS, earlier screening is worth a conversation with your doctor.
Between 44% and 62% of women report cognitive complaints during the menopausal transition [8]. Verbal learning and verbal memory decline specifically from pre- to perimenopause, independent of age.
Oestrogen plays essential roles in neurogenesis, synaptic plasticity, and glucose metabolism in the brain [3, 16]. The critical period hypothesis suggests that oestrogen may confer cognitive benefits when administered during perimenopause or early postmenopause, but that delayed initiation may not help [8]. Andy and colleagues’ 2024 meta-analysis found no significant overall effect on cognition, but identified timing-dependent signals suggesting possible benefit when therapy is initiated early in the menopausal transition [8]. The overall evidence is mixed, and formulation and timing appear to matter considerably.
When I see brilliant, high-functioning women who have come to believe their cognitive decline is anxiety, or depression, or “just getting older”, I am excited by the opportunity to prove them wrong. It is a neurological consequence of hormonal withdrawal, and in many cases it is treatable.
What to consider: If cognitive changes are showing up in your forties, a hormonal assessment alongside any mental health evaluation is a reasonable starting point. Resistance training, sleep quality, and adequate protein intake each have good evidence for supporting brain health in this age group.
Sexual health is not a footnote. For many women, the changes in their sexual function are among the most distressing consequences of the menopausal transition, and among the most treatable. The failure of medicine to address this is a disgrace.
Genitourinary Syndrome of Menopause (GSM) encompasses vaginal dryness, painful sex, recurrent UTIs, urgency, and incontinence [20, 21]. Estimates range from 50-70% of postmenopausal women, with some data putting it at up to 84% six or more years post-menopause [9]. Unlike hot flushes, GSM is progressive. Without treatment, it gets worse and each year of delay makes reversal harder.
Danan and colleagues’ 2024 systematic review (46 RCTs) confirmed that vaginal oestrogen improves vulvovaginal dryness, vaginal DHEA improves both dryness and dyspareunia, and oral ospemifene improves both [10]. Note that ospemifene is not currently TGA-approved in Australia; the locally available options are vaginal oestrogen and vaginal DHEA. Vaginal oestrogen has minimal systemic absorption. It is not systemic HRT. In my view, it’s a conversation worth having for most women entering menopause.
Desire, libido, and testosterone. Islam and colleagues’ meta-analysis of 36 RCTs in Lancet Diabetes and Endocrinology demonstrated that testosterone at physiological doses significantly improves sexual desire, arousal, orgasm, pleasure, and sexual self-image in postmenopausal women [11]. The global consensus position statement supports testosterone therapy at physiological doses for postmenopausal women with hypoactive sexual desire disorder [12]. Glaser and colleagues followed 1,267 women on testosterone for 10 years and found no increased incidence of invasive breast cancer [13]. In Australia, Androfeme 1% is TGA-approved for this indication.
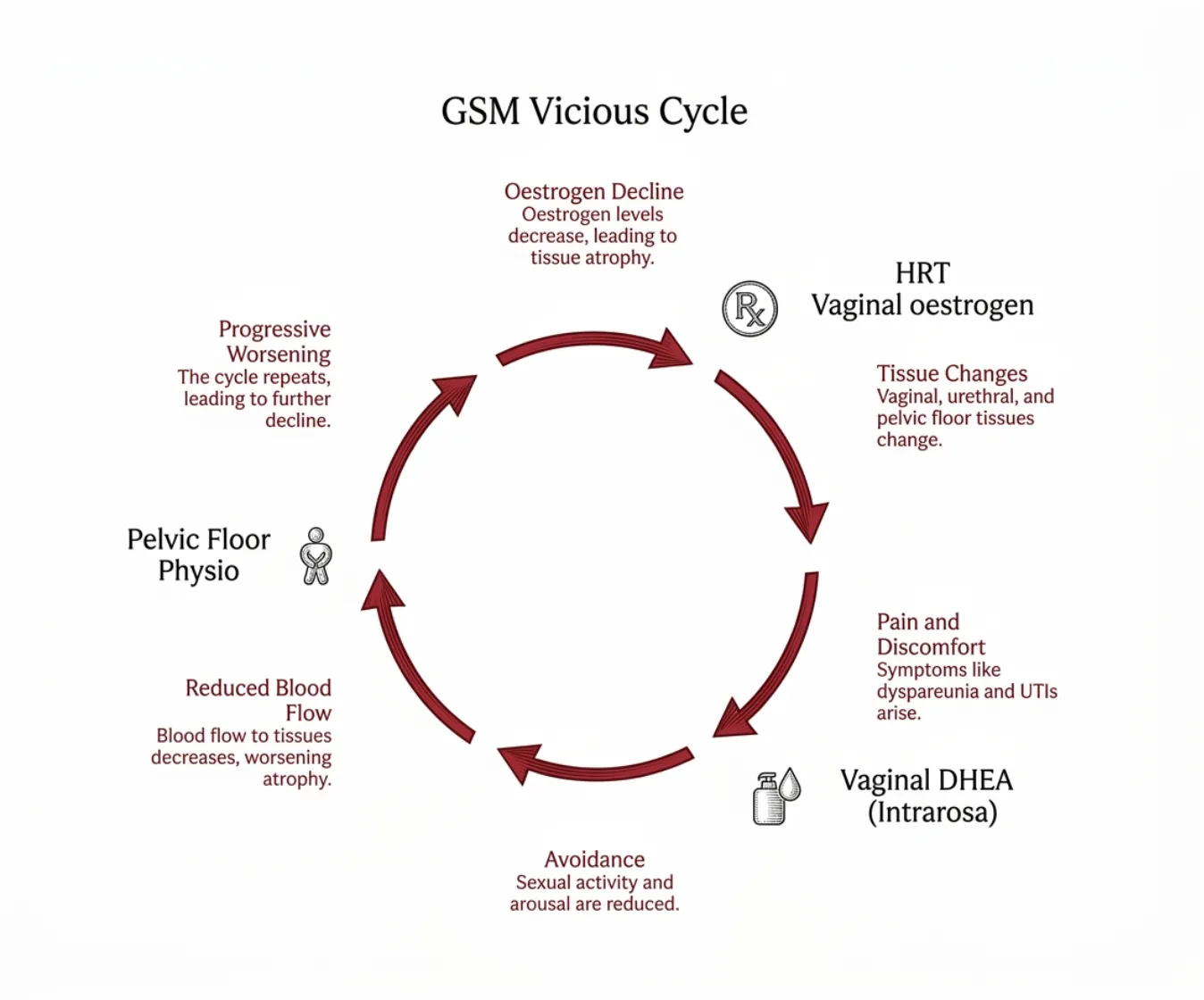
I see the cycle constantly: declining oestrogen leads to vaginal atrophy, which causes painful sex, which reduces desire, which creates avoidance, which strains the relationship. The woman feels broken. The partner feels rejected. And neither has been told this is a predictable, physiological consequence of hormonal change with effective treatments.
What to consider: If sexual health hasn’t come up in your medical conversations, it’s worth raising it. Vaginal oestrogen is a local treatment with minimal systemic absorption [20, 21]. If libido has changed significantly, testosterone at physiological doses is an option supported by good evidence [25, 26]. If sex has become painful, there are medical treatments worth exploring beyond lubricants alone.
Perimenopausal women have approximately 40% higher risk of depression compared to premenopausal women. In the SWAN cohort, women were approximately twice as likely to experience a major depressive episode during perimenopause (OR=2.08), rising to four times more likely in the postmenopausal years (OR=4.32) [14]. Anxiety symptoms are also markedly elevated: a 10-year SWAN cohort study of 2,956 women found approximately 20% of perimenopausal women reported high anxiety, with 56-61% higher odds compared to premenopause [15].
This is neurochemistry, not weakness. Oestrogen upregulates serotonin synthesis, reduces its breakdown by inhibiting MAO-A and MAO-B, and regulates 5-HT1A autoreceptors. Progesterone’s metabolite allopregnanolone is a potent GABA-A modulator with direct anxiolytic properties [16]. When both hormones fluctuate and then decline, the neurochemical architecture of mood regulation is destabilised.
What concerns me is the antidepressant reflex. A woman reports new-onset anxiety or depression in her forties and leaves a consultation with an SSRI and nobody has checked her hormonal status. Gordon and colleagues demonstrated in a double-blind placebo-controlled RCT (n=172, 12 months) that those on placebo were nearly twice as likely to develop clinically significant depressive symptoms compared to those receiving transdermal oestradiol and micronised progesterone (32.3% versus 17.3%) [17]. Langhe’s narrative review reported higher remission rates with transdermal oestradiol compared to placebo in perimenopausal women, though the specific percentages vary across the primary trials cited [16].
The progestogen choice matters. Medroxyprogesterone acetate worsens mood. Norethisterone acetate causes even more pronounced negative symptoms. Micronised progesterone has fewer adverse mood effects [16]. Progestins are not interchangeable.
I am not anti-antidepressant. I am anti-shallow-assessment. If a woman in her late thirties or forties presents with mood changes, hormonal status should be part of the evaluation.
What to consider: If new-onset anxiety or depression appears in your forties, a hormonal assessment alongside any mental health evaluation is a reasonable approach. Gordon’s RCT showed transdermal oestradiol and micronised progesterone nearly halved the rate of depressive symptoms in early perimenopause [17]. If HRT is on the table, the evidence favours micronised progesterone over synthetic progestins [16].
Sleep disturbance affects 16-47% of perimenopausal women and 35-60% of postmenopausal women [18]. The 2am or 3am wake-up that becomes the new normal is the most common complaint I hear.
Declining oestrogen disrupts thermoregulation (hence night sweats), while the loss of progesterone, which has direct sedative properties, compounds the problem [36, 37]. Obstructive sleep apnoea also becomes more prevalent postmenopause, and is systematically underdiagnosed in women because they present differently: more insomnia, more fatigue, less classic snoring as is the case for men [19].
Poor sleep is not a lifestyle inconvenience. It is a clinical accelerant. Thurston’s SWAN data showed that women with persistently disrupted sleep across the menopausal transition had significantly elevated cardiovascular disease risk [20]. It impairs cognition, immune function, and recovery.
What to consider: If regular early waking is a problem, it’s worth looking for a cause rather than simply managing it. If vasomotor symptoms are driving the waking, treating those with HRT often helps the sleep too. CBT-I is first-line for persistent insomnia. A sleep study is worth considering if snoring or apnoea symptoms are present [19].
Women lose up to 20% of their bone mineral density in the five to seven years after menopause [21]. The LIFTMOR trial demonstrated that high-intensity resistance and impact training (heavy deadlifts, squats, overhead press, jumping chin-ups) actually reversed bone loss in postmenopausal women with osteopenia and osteoporosis, not just slowed it [22].
Mohebbi and colleagues synthesised 80 studies (n=5,581) and found that resistance training at 70% or more of one-rep max, three times per week, showed the greatest benefits on bone mineral density [23]. Bone status did not alter the exercise effect, with bones responding regardless.
Combined with adequate vitamin D (50-80% of menopausal women are deficient [24]) and appropriately timed HRT, bone loss is modifiable.
What to consider: A baseline DEXA scan in your early fifties is reasonable, earlier if risk factors are present. Vitamin D is worth checking and supplementing if deficient. Resistance training with progressive overload is the most evidence-based intervention for bone health in this age group.
In 2002, the Women’s Health Initiative published results that terrified an entire generation away from hormone replacement therapy [25]. The WHI enrolled women averaging 63 years old, a full decade past menopause, many with pre-existing cardiovascular risk. They were given oral conjugated equine oestrogen combined with medroxyprogesterone acetate. The study found modest increases in breast cancer and cardiovascular events, and prescriptions dropped by 80% [57, 58].
The WHI’s own 18-year follow-up tells a very different story: HRT was not associated with increased all-cause, cardiovascular, or cancer mortality [26]. Oestrogen-only therapy was associated with reduced breast cancer incidence and mortality over 20 years [27].
The breast cancer question deserves an honest answer. Oestrogen-only therapy (for women who have had a hysterectomy) showed a favourable breast cancer profile [27]. Combined oestrogen plus synthetic progestogen carries a modest increased risk: approximately 1 additional case per 1,000 women per year of use [57, 62]. Body-identical micronised progesterone has a more favourable risk profile than synthetic progestins [42, 63, 65]. Zhang and colleagues’ umbrella review confirmed that risks and benefits depend critically on formulation, route, timing, and duration [28].
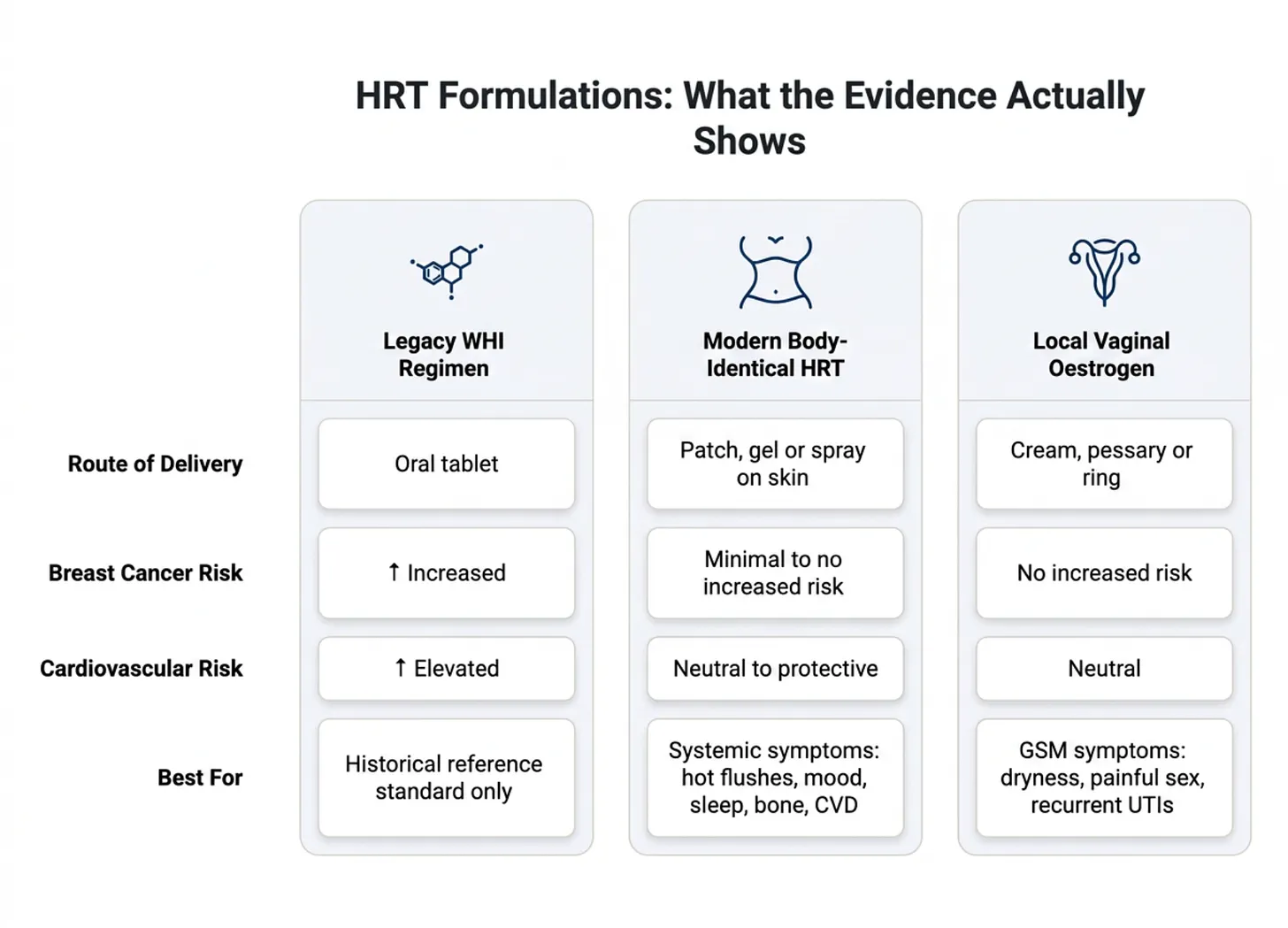
The timing hypothesis is now clear: HRT initiated within 10 years of menopause or before age 60 has a fundamentally different risk-benefit profile than HRT started later [60, 68, 63, 69, 70]. Transdermal oestradiol does not appear to increase venous thromboembolism risk, unlike oral oestrogen [42, 67].
The NAMS 2022 position statement is unambiguous: HRT remains the most effective treatment for vasomotor symptoms and GSM, with the benefit-risk ratio most favourable for women under 60 or within 10 years of menopause [21]. HRT is not appropriate for everyone (active ER-positive breast cancer, active VTE, unexplained vaginal bleeding, active liver disease need individual assessment), but for symptomatic women in the appropriate window, it is a conversation worth having.
What to consider: If symptomatic and within 10 years of menopause or under 60, the evidence supports a conversation about HRT. Transdermal oestradiol and micronised progesterone is the formulation with the most favourable profile for mood, breast, and cardiovascular outcomes [42, 61, 67, 65]. If your GP isn’t familiar with current evidence, a referral to a menopause specialist is a reasonable path.
A note on compounded sublingual (troche) formulations, which are widely prescribed in Australian private practice: troches bypass first-pass liver metabolism and can be effective, but blood levels tend to be highly variable and sometimes supraphysiological. The robust safety evidence around cardiovascular neutrality and breast cancer risk comes predominantly from transdermal studies, and it cannot be directly extrapolated to compounded sublingual products. This is not a reason to avoid them if they are working well for a patient, but it is worth monitoring levels and having an informed conversation with your prescribing doctor about what the evidence does and doesn’t cover.
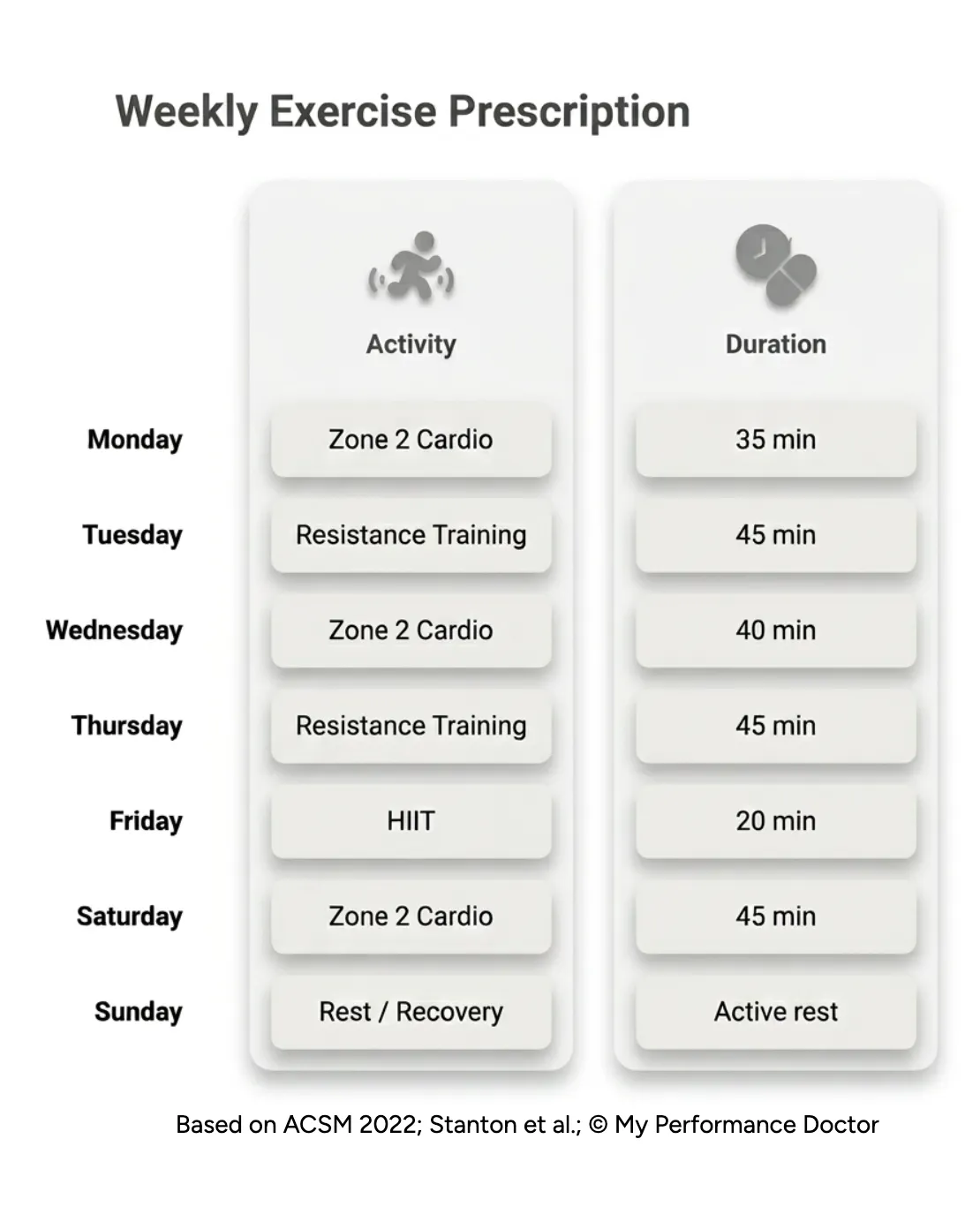
If I could prescribe one thing to every woman in midlife, it would be exercise. But the prescription needs to be specific.
Ji, Gulati, and colleagues analysed over 400,000 participants followed for 22 years: women achieve equivalent all-cause mortality reduction at 140 minutes per week of moderate-to-vigorous physical activity compared to 300 minutes for men. Women who did one session per week of muscle-strengthening exercise achieved similar mortality benefits as men doing three sessions [30]. The dose-response curve is different. Women get more benefit per unit of exercise.
Despite the overwhelming evidence for its benefits, resistance training remains underutilised in this population: preserved bone density, maintained lean mass, reduced vasomotor symptoms, improved cardiovascular risk. Smith-Ryan and colleagues demonstrated that perimenopause represents a critical window for preserving muscle quality, with measurable declines occurring specifically during the perimenopausal transition [31].
Three resistance sessions per week is the target. Two is excellent. One is infinitely better than none. Add 140 minutes of moderate-to-vigorous physical activity per week and one HIIT session, and you have the minimum effective dose for a woman in midlife.
What to consider: Resistance training three times per week with progressive overload gives the best return for bone, metabolic, and cardiovascular health. Around 140 minutes of moderate-to-vigorous activity per week is the target. One HIIT session weekly adds cardiovascular benefit. If you’re currently inactive, one resistance session per week is a meaningful starting point [30].
Feeling like yourself again is not a cosmetic ambition. It is the whole point. Pick one thing: the one with the biggest gap between effort and payoff for you right now. Do it this week. Do it again next week. The rest will follow.


For all media enquiries, please contact press@myperformancedoctor.com
