May 20, 2025
PART 2: What Can Be And Is Being Done About It
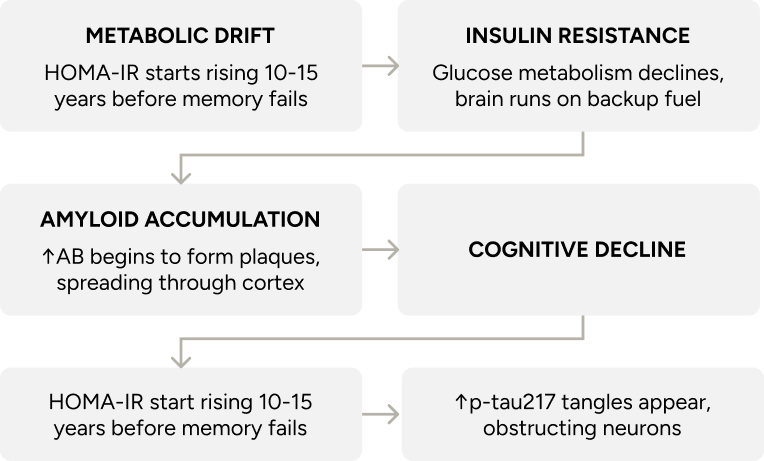
Part 1 explains how Alzheimer’s begins, and just as importantly, when. The earliest changes happen long before memory fades — in how the brain uses energy, manages inflammation, and maintains its structural integrity. These shifts develop gradually and follow recognisable patterns, which means there is time to intervene with purpose.
Part 2 explores five areas where that influence appears strongest: sleep, movement, nutrition, cholesterol, and metabolic health. It ends with a look at emerging treatments designed to ease symptoms while also addressing the disease process itself.
PART 2: What Can Be And Is Being Done About It
Read Time: About 13 minutes
Five levers that alter trajectory if pulled early enough.
Cognitive decline occurs gradually, often preceded by shifts in brain metabolism, inflammation, and neural connections. These early changes tend to follow patterns that respond to input. In systems biology, small forces applied consistently can alter long-term direction⁴⁴ ⁴⁵ ⁴⁶ ⁴⁷.
The following 5 levers, pulled early, appear to reduce risk and preserve function⁴⁶.

Sleep is an active, restorative process during which the brain clears waste, consolidates memories, and resets defences. Deep sleep, especially slow-wave sleep, activates the glymphatic system (a clearance pathway that flushes out neurotoxic proteins like beta-amyloid)⁴⁸.
Sleep to support long-term cognitive function needs to be:

Sufficient: Consistently sleeping 7–8 hours is associated with lower AD risk. Too little is linked to memory loss, mood shifts, and faster cognitive decline⁴⁹.

Efficient: Sleep efficiency above 85% is linked to better memory and reduced amyloid-beta, a key Alzheimer’s factor⁵⁰. Lower sleep efficiency correlates with higher amyloid-beta in healthy older adults⁵¹.

Regular: Irregular bed and wake times disrupt circadian rhythms, which regulate amyloid clearance and synaptic repair. This instability has been linked to the earlier onset of AD symptoms⁵².
Multiple factors shape sleep architecture. Tracking tools now reveal patterns in efficiency⁵³, fragmentation⁵⁴, and sleep stages⁵⁵. Evening light, caffeine, or alcohol disrupt timing by delaying melatonin secretion and suppressing deep sleep.⁵⁶

Physical training supports the growth of new neurons, enhances mitochondrial function, and improves metabolic health.⁵⁷ Regular exercise has been linked to significantly lower AD risk and improved cognitive performance across the lifespan.⁵⁸
What to train to reduce AD risk:

Aerobic Capacity: Moderate-intensity exercise (at 60–70% of maximum heart rate) improves memory and executive function — even a single 30-minute session can have measurable effects⁵⁹ ⁶⁰.

Muscle Strength: Moderate-to-high intensity resistance training regularly enhances cognitive function and is associated with functional improvements in the frontal lobe⁶¹ ⁶².

Cognitive-Motor Integration: Dual-task exercises, combining movement with mental challenge, improve brain function and physical capacity.For instance, simultaneous walking and counting backwards requires attention and motor coordination, significantly enhancing cognitive flexibility and gait stability in older adults⁶³.

Neuromuscular Control: Balance and coordination training engages cognitive circuits; even one session can sharpen attention in older adults. An example is the practice of Tai Chi, a mind–body exercise that integrates physical movement with cognitive concentration⁶⁴.

Specific dietary patterns and nutrients can reduce neuroinflammation, improve synaptic plasticity and metabolic pathways, impacting cognitive health and AD risk⁶⁵. In particular, the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) showed that combining diet, exercise, cognitive training, and vascular monitoring can maintain or improve cognition in older adults at risk of decline⁶⁶.
Specific nutritional interventions that may reduce AD risk:

MIND Diet: The Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diet combines the Mediterranean and Dietary Approaches to Stop Hypertension (DASH) diets, emphasising plant-based foods like leafy greens, berries, nuts, and whole grains, while limiting red meat, butter, and sweets. This dietary pattern has been linked to slower cognitive decline and a reduced risk of Alzheimer’s disease⁶⁷.

Ketogenic Diet: A high-fat, low-carbohydrate diet that shifts the body’s metabolism to use ketone bodies as an alternative energy source. This approach may improve cognitive function, particularly in individuals with insulin resistance or those carrying the ApoE ε4 allele⁶⁸.

Docosahexaenoic Acid (DHA): One of the two long-chain omega-3 fatty acids supports neuron structure and is linked to better cognition and lower AD risk⁶⁹.
Polyphenols: Plant compounds that reduce neuroinflammation and support brain health.⁷⁰ The best, most accessible forms are found in dark fruits, green tea, dark chocolate, olive oil, and various herbs and spices.

B Vitamins: B6, B9, and B12 lower homocysteine, which is linked to slower brain atrophy in mild cognitive impairment⁷¹.

Time-Restricted Eating: Involves consuming all daily calories within a specific time window, such as 8–12 hours, but other common intervals include shorter windows like 6-hour or 10-hour eating periods. Aligning food intake with circadian rhythms through these fasting intervals may enhance brain function, reduce inflammation, and improve sleep quality, potentially benefiting individuals at risk for AD⁷².

Advanced lipid profiling reveals patterns linked to cognitive decline—even in individuals with “normal” total cholesterol⁷³. Smaller, denser LDL particles are more likely to oxidise and breach the blood–brain barrier. Mendelian randomisation (MR) studies confirm that elevated triglycerides are causally linked to cognitive impairment, likely through insulin resistance mechanisms and compromised vascular health⁷⁴ ⁷⁵.
Similarly, higher HDL cholesterol levels appear protective against cognitive decline according to genetic evidence. High lipoprotein(a), a genetically determined LDL variant, is associated with increased risk of stroke and white matter lesions. However, MR studies have not established a direct causal role in Alzheimer’s disease⁷⁶.
As a result, lipid targets now converge across cardiovascular and neurological domains⁷⁷. Thresholds associated with long-term brain health include LDL below 1.8 mmol/L,⁷⁸ HDL above 1.6 mmol/L,⁷⁹ triglycerides under 1.1 mmol/dL,⁸⁰ and Lp(a) below 75 nmol/L⁸¹ — values that define a lipid environment optimised for synaptic stability, vascular integrity, and cognitive resilience⁸².

The most sensitive markers of early metabolic change linked to cognitive decline are fasting insulin, HbA1c, and the glucose tolerance test (which is why I test these in every patient at regular intervals). They reflect how efficiently the body processes glucose at rest. Even modest elevations in these values have been linked to reduced cerebral glucose metabolism, increased amyloid burden, and impaired executive function⁸³ ⁸⁴.
Values associated with metabolic stability — and by extension, cognitive protection — include HbA1c below 5.5%, fasting insulin under 5 µIU/mL, and HOMA-IR below 1.5. Continuous glucose monitoring captures postprandial spikes and daily variability that static labs often miss, offering a more dynamic view of glucose regulation under real-world conditions. Lipoprotein profiling adds further resolution, linking metabolic flexibility with long-term structural and cognitive integrity⁸⁵.
Figure 3. Five Levers for Alzheimer’s Prevention
These five domains, sleep, movement, nutrition, cholesterol, and metabolic markers, represent modifiable inputs that shape long-term cognitive trajectory. Each influences key biological processes implicated in early Alzheimer’s pathology, including toxin clearance, synaptic resilience, and insulin sensitivity. When addressed early and consistently, they offer leverage points for delaying or reducing disease onset.
SLEEP

Enables toxin clearance
Aim for 7-8 hours per night
MOVEMENT

Improves metabolic health
Do 150+ minutes of exercise weekly
NUTRITION

Supports brain function
Follow the MIND diet
CHOLESTEROL

Helps stabilise neurons
Keep LDL < 70 mg/dL
BLOOD MARKERS

Tracks metabolic shifts
Keep HbA1c < 5.5%
The Future of AD Treatment: Leading Research and Emerging Therapies
If you’d asked me ten years ago what we had for Alzheimer’s, I would’ve said donepezil, and that’s it. It offered symptomatic relief, particularly in early stages, but did not affect the disease’s progression or underlying pathology⁸⁶. Now, the field is gaining traction with interventions that match the complexity of the disease.
Today, AD is a field of entrance research, and there is optimism that a cure or at very least an effective treatment will be available within 10 years. Here are some of the approaches scientists and clinicians are taking:
ApoE4-Targeted Approaches
Several new approaches specifically target ApoE4 biology, either by reducing its production, modifying its genetic code, or counteracting its downstream effects. The table below outlines leading interventions currently under investigation:
Table 2. Emerging Alzheimer’s Interventions by Mechanism and Development Stage
This table outlines promising therapies targeting diverse mechanisms implicated in Alzheimer’s disease, from genetic regulation to metabolic resilience. Each intervention is categorised by its current phase of development:
- Preclinical: Therapies still in laboratory or animal studies. These are early-stage concepts undergoing safety, efficacy, and mechanism validation before testing in humans.
- Clinical: Interventions already being tested in humans across varying trial phases.
Together, these entries reflect the field’s movement toward targeted, mechanism-based approaches that address Alzheimer’s at its roots.
INTERVENTION
IONIS-APOE4Rx⁸⁷
DEVELOPMENT STAGE
Preclinical
BIOLOGICAL TARGET AND RATIONALE
Apolipoprotein E4 (ApoE4) — this protein variant is strongly associated with Alzheimer’s risk through its effects on amyloid accumulation, neuroinflammation, and lipid metabolism.
HOW IT WORKS
Uses antisense oligonucleotides, which are short synthetic strands of nucleic acid designed to bind ApoE4’s messenger RNA. This blocks the cell’s ability to “read” the blueprint and prevents the protein from being made, like silencing a bad instruction before it becomes a faulty machine.
THERAPEUTIC GOAL
Prevents the chain of biochemical disruptions linked to ApoE4 — offering a disease-modifying approach for genetically at-risk individuals.
INTERVENTION
ApoE4 Gene Editing⁸⁸
DEVELOPMENT STAGE
Preclinical
BIOLOGICAL TARGET AND RATIONALE
APOE ε4 allele — the single most important genetic risk factor for late-onset Alzheimer’s. Modifying it could shift the entire disease trajectory.
HOW IT WORKS
Applies CRISPR-based base editing, a next-generation tool that changes one DNA letter without cutting the strand. This converts ε4 into the lower-risk ε3 version, effectively “rewriting” the inherited instructions at their source.
THERAPEUTIC GOAL
Transforms a static genetic risk into a modifiable factor — with potential lifelong impact on Alzheimer’s susceptibility.
INTERVENTION
CM-414⁸⁹
DEVELOPMENT STAGE
Preclinical
BIOLOGICAL TARGET AND RATIONALE
HDAC and PDE5 enzymes — these control how neurons express genes and relay signals. Their dysfunction in AD impairs synaptic plasticity, a core component of learning and memory.
HOW IT WORKS
Inhibits HDACs (which normally tighten DNA and suppress gene activity) to unlock expression of key memory genes, and blocks PDE5 to enhance cyclic GMP signalling — a vital pathway for neural communication. Together, they reboot the brain’s learning circuitry.
THERAPEUTIC GOAL
Repairs synaptic connections and restores the brain’s ability to adapt — especially important in individuals with ApoE4-related impairments.
INTERVENTION
T3D-959⁹⁰
DEVELOPMENT STAGE
Clinical (Phase 2)
BIOLOGICAL TARGET AND RATIONALE
PPAR-delta and PPAR-gamma receptors — nuclear sensors that regulate how brain cells process glucose and lipids. These are impaired early in AD, especially in ApoE4 carriers.
HOW IT WORKS
Activates both receptors to normalise energy production in neurons. PPAR-delta improves mitochondrial efficiency and anti-inflammatory signalling, while PPAR-gamma enhances insulin sensitivity and lipid metabolism.
THERAPEUTIC GOAL
Restores neuronal fuel supply and reduces metabolic strain — potentially preserving cognitive performance in early or mild disease.
INTERVENTION
GLP-1 receptor agonists⁹¹
DEVELOPMENT STAGE
Clinical (Early phase)
BIOLOGICAL TARGET AND RATIONALE
Brain insulin signalling — critical for neuronal energy balance and survival. It becomes blunted in Alzheimer’s, mimicking insulin resistance seen in diabetes.
HOW IT WORKS
Stimulates GLP-1 receptors, enhancing the brain’s response to insulin and increasing glucose uptake. Also reduces inflammation and oxidative stress, which further preserves neural health.
THERAPEUTIC GOAL
Keeps neurons nourished and metabolically resilient — a possible defence against early decline in cognition and function.
INTERVENTION
MAP – Metformin
DEVELOPMENT STAGE
Clinical (Large-scale trial)
BIOLOGICAL TARGET AND RATIONALE
Insulin resistance in the brain is one of the earliest and most treatable abnormalities in Alzheimer’s progression.
HOW IT WORKS
Activates AMPK, a master energy sensor, which improves how neurons handle glucose and fatty acids. This lowers inflammation and increases energy efficiency, like tuning an engine to run cleaner and longer.
THERAPEUTIC GOAL
Delays the onset or slows progression of cognitive decline by maintaining energy availability and reducing inflammatory stress in the brain.
INTERVENTION
ALZ-801⁹²
DEVELOPMENT STAGE
Clinical (Phase 3)
BIOLOGICAL TARGET AND RATIONALE
Amyloid beta oligomers are soluble, early-stage aggregates of amyloid that are more neurotoxic than plaques. They impair synaptic function long before symptoms appear.
HDL-mediated cholesterol transport is disrupted in ApoE4 carriers, leading to membrane instability and impaired synaptic repair.
HOW IT WORKS
Stabilises amyloid precursor protein (APP) to prevent it from fragmenting into toxic oligomers. Unlike plaque-clearing antibodies, it acts upstream to stop the problem before it starts.
THERAPEUTIC GOAL
Reduces neuronal damage and synaptic loss — aiming for better cognitive preservation with fewer inflammatory side effects.
INTERVENTION
CETP Inhibition⁹³
DEVELOPMENT STAGE
Clinical (Early Phase)
BIOLOGICAL TARGET AND RATIONALE
HDL-mediated cholesterol transport is disrupted in ApoE4 carriers, leading to membrane instability and impaired synaptic repair.
HOW IT WORKS
Inhibits cholesteryl ester transfer protein (CETP), increasing HDL function and improving lipid redistribution within the brain. This supports healthier membranes and neurotransmission.
THERAPEUTIC GOAL
Restores lipid balance in the brain, especially in individuals with genetically driven transport deficits, potentially slowing neurodegeneration.
INTERVENTION
Senolytics⁹⁴
DEVELOPMENT STAGE
Clinical (Early Phase)
BIOLOGICAL TARGET AND RATIONALE
Senescent glial cells — metabolically active but non-dividing- release inflammatory molecules that damage surrounding tissue and drive neurodegeneration.
HOW IT WORKS
Uses small molecules that induce apoptosis (programmed cell death) in senescent cells without affecting healthy ones. This purges inflammatory cells and clears the way for tissue repair.
THERAPEUTIC GOAL
Reduces chronic inflammation in the brain’s support cells, creating a cleaner, more functional environment for long-term neuronal survival.
Leading Centres of Excellence
The fight against Alzheimer’s now operates a global network of specialised research centres collaborating across disciplines. Breakthroughs in one area rapidly inform progress in others. From molecular mechanisms to clinical applications, this model accelerates discoveries beyond what any single centre could achieve.






These centres collaborate through networks like the Alzheimer’s Disease Research Centers (ADRCs) and the Alzheimer’s Disease Neuroimaging Initiative (ADNI), creating platforms where data sharing accelerates discovery across the entire field.
From Genetic Risk to Proactive Prevention
Alzheimer’s disease represents a convergence of genetic predisposition, metabolic dysfunction, and environmental factors that disrupt fundamental mechanisms of brain health long before symptoms arise.
While the presence of the ApoE ε4 allele increases susceptibility, its trajectory is neither deterministic nor irreversible. Early intervention targeting metabolic stability, lipid management, sleep optimisation, and neuroinflammation offers the best defence against cognitive decline.
As our diagnostic capabilities expand and targeted therapies evolve, the paradigm shifts from passive observation to proactive prevention. Clinicians need to lead this shift by giving patients the tools and knowledge to protect their brain health for life.
From Drift to Dementia
Medical Disclaimer
The information provided by My Performance Doctor on this website, including written content, videos, and other materials, is intended solely for general informational and educational purposes. It does not constitute medical advice, diagnosis, or treatment and should not be relied upon as a substitute for professional medical judgment.
Using this site or its content does not create a doctor-patient relationship. Any application of the information provided is at the user’s own discretion and risk.
You should not delay or disregard seeking medical advice based on anything you read or view here. Always consult your healthcare provider regarding any medical concerns, symptoms, or conditions.

ABOUT THE AUTHOR
For over 30 years, Dr. Weisinger has been dedicated to improving health, performance, and well-being. His expertise spans clinical care, research, and academic instruction. Discover why so many trust Dr. Weisinger for personalised, proactive healthcare—because true health is about thriving, not just surviving.